The sacroiliac joint (SIJ) is a common site of dysfunction and pain generation in the lumbo-pelvic spine. Various types of analyses have been utilized in the chiropractic profession to assess the SIJ in the guidance of applying proper therapeutic and corrective adjustment techniques. Below are several ways of testing the mobility of the SIJ in the standing position that can be easily incorporated into daily practice.
Note: All descriptions for unilateral tests will be for the right side. In practice repeat these on the left.
Load Transfer Test for Pelvic Stability
With the patient standing unsupported, contact their right PSIS and the S2 tubercle. Have the patient lift their left (opposite) leg 3-4 inches. The PSIS should remain still or move slightly inferiorly. If the PSIS (illium) moves cephalad or rotates anteriorly relative to the sacrum, it indicates possible SIJ and pelvic instability. Note: if the patient is unable to maintain good balance during this test, the results aren’t valid.

Gillet Test for Intrapelvic Mobility
This tests the ability of the ilium to flex and extend on the sacrum. There are four movements for each side, with the patient standing and supporting themselves.
Upper Right Flexion: Contact their right PSIS and the S2 tubercle. Have the patient lift their right knee as far to their chest as they comfortably can without compromising their balance. Normally, the right PSIS moves down and out.
Upper Right Relative Extension: Using the same contact points, have the patient lift their left (opposite) knee to their chest as they comfortably can without compromising their balance. Normally, the S2 moves down relative to the right PSIS.
Lower Right Flexion: Contact their right PIIS and the S4 tubercle. Have the patient lift their right knee as far to their chest as they comfortably can without compromising their balance. Normally, the right PIIS moves down and out.
Lower Right Relative Extension: Using the same contact points, have the patient lift their left (opposite) knee to their chest as they comfortably can without compromising their balance. Normally, the right S4 moves down relative to the right PIIS.
In all these tests make sure that the ilium doesn’t translate superior with hip flexion, and that there isn’t excessive weight shifting toward the back or onto the supporting leg side. If the patient has difficulty maintaining balance doing these movements, consider the possibility of lower extremity dysfunction or instability, or poor neuromuscular coordination.


Standing Forward Flexion Test for Lumbo-Pelvic Mobility:
With the patient standing unsupported, contact both their PSISs. Have them bend forward as far they comfortably can keeping their knees locked in extension..
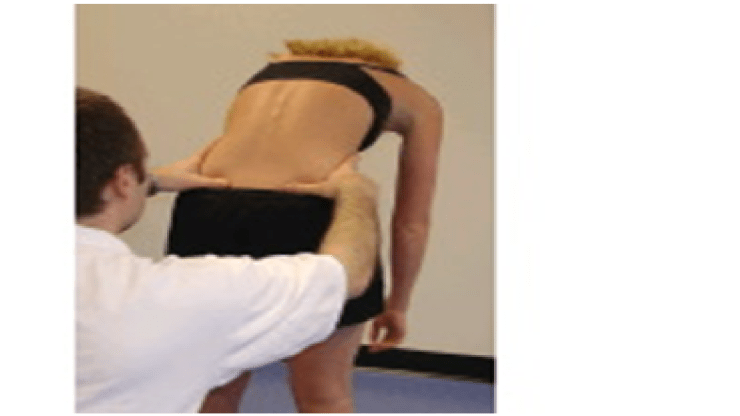
Normally the PSIS should be stable on flexion. If one of the PSIS moves superior (anterior innominate rotation), it indicates the side of dysfunctional SIJ. If the test produces pain, return to the starting position and repeat it while unloading the possible involved structure in the following manner:
First, compress the SIJ to support an unstable pelvis. Next, repeat while compressing the Quadratus Lumborum (QL). Lastly, repeat holding each ilium in a posterior-inferior position. This will help distinguish if the dysfunction is due to a fixated SIJ, hypermobile SIJ, hypertonicity of the QL on the positive side, or hamstring tightness on the opposite side. Finally, look for any alteration of lumbopelvic rhythm.
About The Author
Dr. David Graber is the chairperson of the ANJC Council on Technique and Clinical Excellence, and maintains a private practice in Mountain Lakes, NJ. He can be reached at: GraberDC@aol.com.
(Published in The New Jersey Chiropractor, Winter 2016, Vol.12, No. 1)
